Despite Reading Numerous Research Studies That Report the Association of Fast Food
Americans with more pedagogy alive longer, healthier lives than those with fewer years of schooling (see Result Brief #1). But why does education thing so much to wellness? The links are complex—and tied closely to income and to the skills and opportunities that people have to atomic number 82 healthy lives in their communities.
How are health and instruction linked? In that location are three main connections:ane
- Didactics can create opportunities for better health
- Poor health tin can put educational attainment at run a risk (reverse causality)
- Conditions throughout people's lives—showtime in early childhood—can affect both health and instruction
Read More
This issue brief, created with back up from the Robert Wood Johnson Foundation, provides an overview of what research shows nigh the links between education and health alongside the perspectives of residents of a disadvantaged urban community in Richmond, Virginia. These community researchers, members of our partnership, interact regularly with the Center on Society and Health's research and policy activities to help united states more fully understand the "existent life" connections betwixt community life and health outcomes.
1. The Health Benefits of Education
Income and Resources

"Being educated now means getting ameliorate employment, didactics our kids to be successful and just making a difference in, just in everyday life." —Brenda
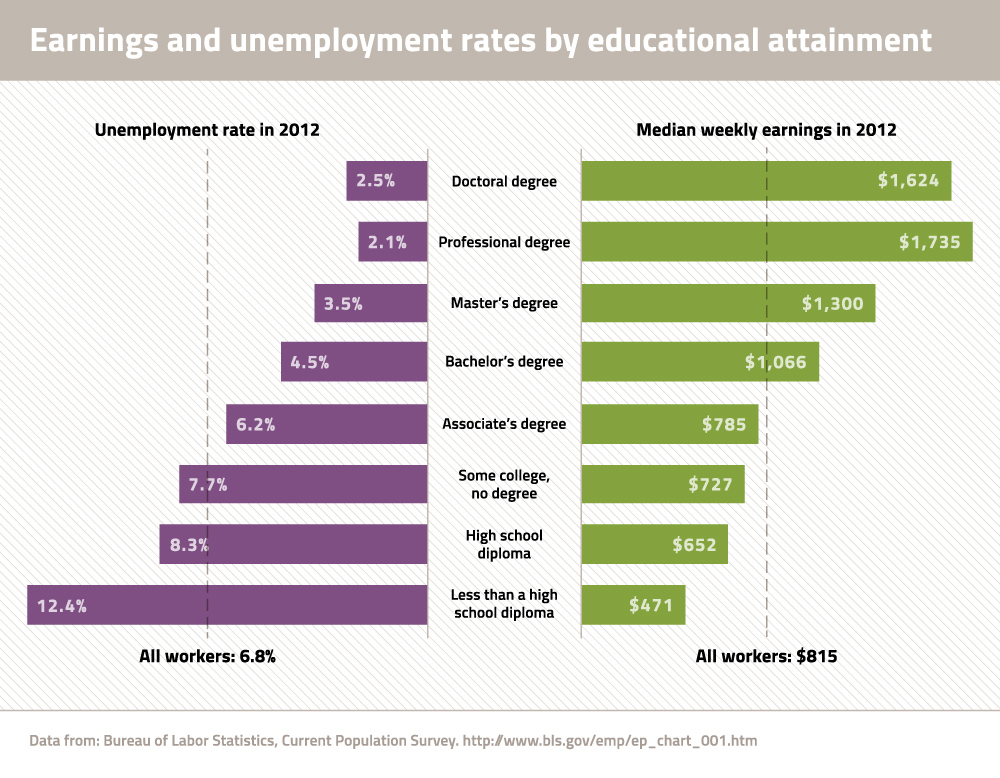
Better jobs: In today's knowledge economic system, an bidder with more pedagogy is more likely to be employed and land a job that provides health-promoting benefits such as wellness insurance, paid leave, and retirement.5 Conversely, people with less education are more likely to work in high-risk occupations with few benefits.
College earnings: Income has a major effect on health and workers with more than education tend to earn more money.2 In 2012, the median wage for college graduates was more than twice that of high school dropouts and more than one and a half times higher than that of loftier schoolhouse graduates.6 Read More

"Definitely having a good teaching and a good paying chore can salve a lot of mental stress."
—Chimere
Resources for good health: Families with higher incomes can more than hands purchase healthy foods, have time to do regularly, and pay for health services and transportation. Conversely, the task insecurity, low wages, and lack of assets associated with less education can brand individuals and families more vulnerable during hard times—which can pb to poor nutrition, unstable housing, and unmet medical needs. Read More

Social and Psychological Benefits

"So through school, we learn how to socially engage with other classmates. We larn how to engage with our teachers. How nosotros speak to others and how we permit that to grow equally we get older allows us to learn how to ask those questions when we're working within the healthcare organization, when we're working with our doctor to understand what is going on with us."
—Chanel
Reduced stress: People with more education—and thus higher incomes—are often spared the health-harming stresses that accompany prolonged social and economic hardship. Those with less teaching ofttimes have fewer resources (east.1000., social back up, sense of control over life, and loftier self-esteem) to buffer the effects of stress. Read More than
Social and psychological skills: Education in school and other learning opportunities outside the classroom build skills and foster traits that are important throughout life and may be important to wellness, such as conscientiousness, perseverance, a sense of personal command, flexibility, the capacity for negotiation, and the power to form relationships and establish social networks. These skills can assist with a multifariousness of life'south challenges—from work to family unit life—and with managing one's wellness and navigating the health care arrangement. Read More
Social networks: Educated adults tend to have larger social networks—and these connections bring access to fiscal, psychological, and emotional resources that may aid reduce hardship and stress and better health. Read More
"Being able to advocate and ask for what you lot want, helps to facilitate a healthier lifestyle. … If it'due south needing your community to have green spaces, have a park, a playground, take amend trails within the community, advocating for that will aid."
—Chanel
Health Behaviors
Knowledge and skills: In addition to being prepared for better jobs, people with more than pedagogy are more likely to learn well-nigh healthy behaviors. Educated patients may be more able to understand their wellness needs, follow instructions, advocate for themselves and their families, and communicate finer with wellness providers.21 Read More
Healthier Neighborhoods

"Poor neighborhoods oftentimes lead to poor schools. Poor schools lead to poor education. Poor instruction oftentimes leads to poor work. Poor piece of work puts you right back into the poor neighborhood. It's a vicious cycle that happens in communities, especially inner cities." —Albert
Lower income and fewer resources mean that people with less education are more likely to live in low-income neighborhoods that lack the resources for skilful health. These neighborhoods are ofttimes economically marginalized and segregated and have more than hazard factors for poor health such as:
- Less admission to supermarkets or other sources of healthy nutrient and an crowd of fast food restaurants and outlets that promote unhealthy foods.25
Read More

"If the best affair that you lot come across in the neighborhood is a drug dealer, then that becomes your goal. If the all-time affair you encounter in your neighborhood is working a ix to five, then that becomes your goal. Merely if you lot meet the doctors and the lawyers, if you see the teachers and the professors, so that becomes your goal." —Marco

"It's a lot of things going on [in this customs], a lot of challenges. It's but hard sometimes to endeavour and get people to come up together, as 1, merely so we can solve the problem." —Toni
- Less greenish space, such as sidewalks and parks to encourage outdoor physical activity and walking or cycling to work or school.
- Rural and depression-income areas, which are more than populated past people with less pedagogy, oft suffer from shortages of primary care physicians and other health intendance providers and facilities.
- Higher law-breaking rates, exposing residents to greater risk of trauma and deaths from violence and the stress of living in unsafe neighborhoods. People with less education, particularly males, are more probable to be incarcerated, which carries its ain public health risks.
- Fewer high-quality schools, frequently considering public schools are poorly resourced by depression holding taxes. Low-resourced schools have greater difficulty offering attractive teacher salaries or properly maintaining buildings and supplies.
- Fewer jobs, which can exacerbate the economic hardship and poor health that is common for people with less didactics.
- Higher levels of toxins, such as air and water pollution, hazardous waste, pesticides, andindustrial chemicals.27
- Less effective political influence to abet for community needs, resulting in a persistent bike of disadvantage.
2. Poor Health That Affects Education (Reverse Causality)
"Things that happen in the habitation can definitely affect a child being able to even concentrate in the classroom. … If you're hungry, yous can't learn with your abdomen growling. … If you're worried well-nigh your mom existence safe while you're at schoolhouse, you're not going to exist able to pay attention." —Chimere
The relationship between education and health is never a simple one. Poor health not only results from lower educational attainment, it tin too crusade educational setbacks and interfere with schooling.
For example, children with asthma and other chronic illnesses may experience recurrent absences and difficulty concentrating in class.28 Disabilities can besides bear on schoolhouse performance due to difficulties with vision, hearing, attending, behavior, absenteeism, or cognitive skills. Read More than
3. Conditions Throughout the Life Course—Starting time in Early Childhood—That Affect Both Health and Education
A third way that education can be linked to health is by exposure to conditions, commencement in early childhood, which tin can affect both education and health. Throughout life, conditions at domicile, socioeconomic condition, and other contextual factors tin create stress, cause illness, and deprive individuals and families of resources for success in schoolhouse, the workplace, and salubrious living. Read More
What about social policy?
Social policy—decisions almost jobs, the economy, instruction reform, etc.—is an important driver of educational outcomes AND affects all of the factors described in this cursory. For example, underperforming schools and bigotry affect not only educational outcomes only also economic success, the social surround, personal behaviors, and access to quality health care. Social policy affects the didactics organization itself but, in addition, individuals with low educational attainment and fewer resource are more than vulnerable to social policy decisions that bear on access to health intendance, eligibility for assist, and support services.
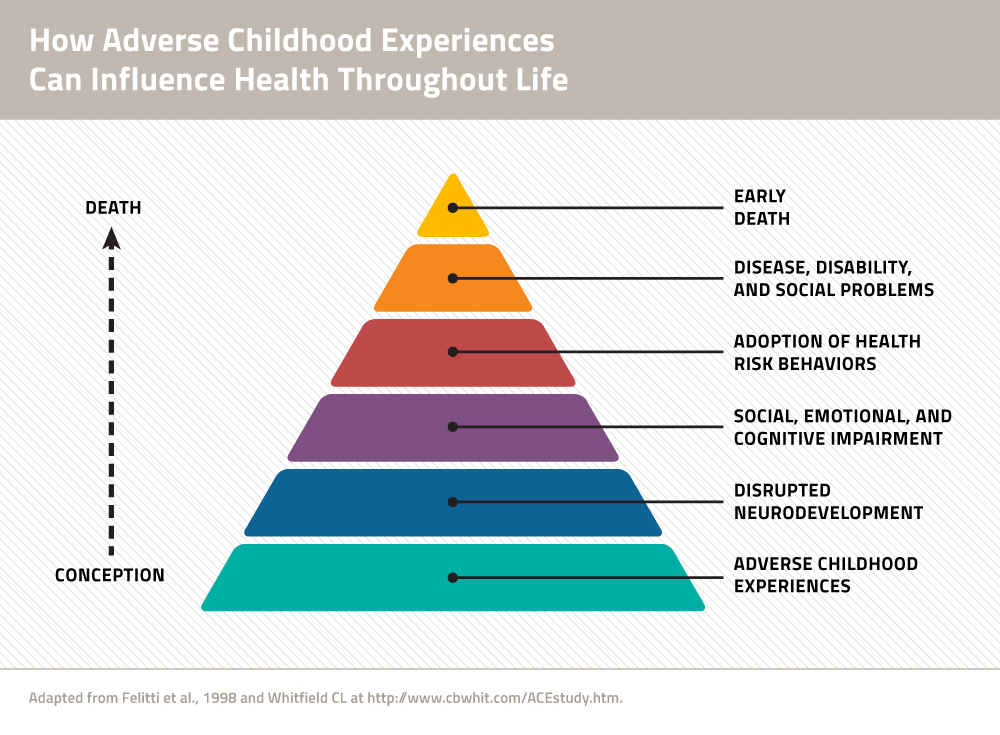
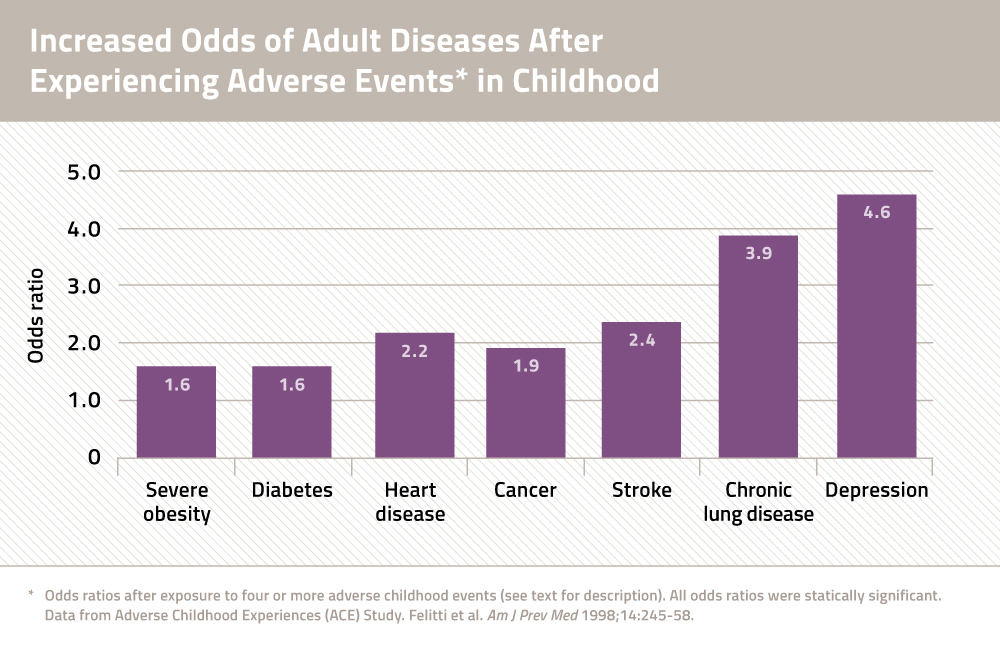
A growing body of research suggests that chronic exposure of infants and toddlers to stressors—what experts phone call "adverse childhood experiences"—can bear upon brain evolution and disturb the child'southward endocrine and immune systems, causing biological changes that increase the risk of centre disease and other weather later in life (come across Graphic 1). For case:
"The connectedness that I will say between education and wellness would exist a good for you mind produces a healthy person. A motivated mind produces a motivated person. A curious listen produces a curious person. When yous have those things it drives yous to desire to know more, to desire to have more, to want to ask more. And when y'all desire more than, yous volition get more. You know where the mind goes the person follows… and that includes health." —Marco
- The adverse effects of stress on the developing encephalon and on beliefs can affect performance in school and explain setbacks in educational activity. Thus, the correlation between lower educational attainment and illness that is later observed amongst adults may accept every bit much to do with the seeds of illnessand inability that are planted earlier children ever reach school age every bit witheducation itself.
- Children exposed to stress may likewise be drawn to unhealthy behaviors—such as smoking or unhealthy eating—during adolescence, the age when adult habits are ofttimes first established.
Read More than
What about individual characteristics?
Characteristics of individuals and families are important in the relationship between education and health. Race, gender, age, inability and other personal characteristics ofttimes affect educational opportunities and success in school (see Event Brief #1). Discrimination and racism have multiple links to education and health. Racial segregation reduces educational and job opportunities51 and is associated with worse wellness outcomes.52, 53
How does education bear on wellness in your customs?
The Middle on Society and Health (CSH) worked with members of Engaging Richmond, a community-bookish partnership that included residents of the East End, a disadvantaged neighborhood of Richmond, Virginia. This inquiry into the links between education and health was a pilot study to learn how individuals could add to our agreement of this complex effect using the lens of their own experiences.
What does your community accept to say virtually the links between didactics and wellness – or other wellness disparities? Learn more about community research partnerships and customs engagement:
- Principles of Community Engagement, 2nd Edition
- Community Campus Partnerships for Health
- Community Engaged Scholarship Toolkit
- AHRQ — The Role of Community-Based Participatory Inquiry
- CSH'south Customs University Partnership
References
- Cutler D., and Lleras-Muney A. Education and Health. In: Anthony J. Culyer (ed.), Encyclopedia of Health Economics, Vol 1. San Diego: Elsevier; 2014. pp. 232-45.
- Olshansky SJ, et al. Differences in life expectancy due to race and educational differences are widening, and many may not grab up. Health Aff 2012;31:1803-xiii.
- Goldman D, Smith JP. The increasing value of education to wellness. Soc Sci Med 2011;72:1728-37.
- Montez JK, Berkman LF. Trends in the educational gradient of bloodshed among Usa adults aged 45 to 84 years: bringing regional context into the explanation. Am J Public Health 2014;104:e82-xc.
- Baum S, Ma J, Payea One thousand. Education Pays 2013: The Benefits of Higher Education for Individuals and Society. College Board, 2013.
- Current Population Survey, U.S. Department of Labor, U.South. Bureau of Labor Statistics. Accessed 4/ix/fourteen at http://www.bls.gov/emp/ep_table_001.htm.
- Julian TA and Kominski RA. Teaching and Synthetic Work- Life Earnings Estimates. American Customs Survey Reports, ACS-14. Washington, DC: U.S. Census Agency, 2011.
- Sobolewski JM, Amato PR. Economic hardship in the family of origin and children's psychological well-being in adulthood. J Marriage Fam 2005;67:141-56.
- Centers for Disease Command, Office of Surveillance, Epidemiology, and Laboratory Services. Behavioral Risk Cistron Surveillance Arrangement, 2010 BRFSS Data. Accessed Feb 14, 2014 at http://www.cdc.gov/brfss/data_tools.htm
- Steele CB, et al. Colorectal Cancer Incidence and Screening – United States, 2008 and 2010. CDC Health Disparities and Inequalities Report — U.s.a., 2013. Centers for Disease Control. MMWR 2013;62(3):53-sixty.
- Mcewen BS, Stellar East. Stress and the individual: mechanisms leading to affliction. Arch Int Med 1993;153:2093-101.
- Karlamangla Equally, et al. Reduction in allostatic load in older adults is associated with lower all-cause bloodshed risk. Psychosom Med 2006;68:500–seven.
- Ross CE, Wu CL. The links between instruction and health. Am Soc Rev 1995;60:719-45.
- Roberts BW, et al. The power of personality: The comparative validity of personality traits, socioeconomic status, and cerebral ability for predicting of import life outcomes. Perspect Psychol Sci 2007;2:313-45.
- Heckman JJ, Kautz T. Hard evidence on soft skills. Labour Economics 2012;nineteen:451-64.
- Berkman LF. The role of social relations in health promotion. Psychosom Med 1995;57:245-54.
- Ross CE, Mirowsky J. Refining the association between didactics and health: the effects of quantity, credential, and selectivity. Census 1999;36:445-60.
- Kaplan GA, et al. Social functioning and overall bloodshed: Prospective evidence from the Kuopio Ischemic Heart Disease Risk Factor Study. Epidemiology 1994;5:495-500.
- Seeman TE. Social ties and health: the benefits of social integration. AEP 1996;vi:442-51.
- Sum A, et al. The Consequences of Dropping Out of High School: Joblessness and Jailing for Loftier School Dropouts and the High Cost for Taxpayers. Center for Labor Market place Studies, Northeastern University, Boston, 2009.
- Goldman DP, Smith JP. Tin can patient self-direction help explain the SES wellness gradient? Proc Natl Acad Sci 2002;10929–10934.
- Spandorfer JM, et al. Comprehension of discharge instructions by patients in an urban emergency section. Ann Emerg Med 1995;25:71-4.
- Williams MV, et al. Inadequate literacy is a barrier to asthma noesis and self-care. Breast 1998;114:1008-15.
- Berkman ND, et al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med 2011;155:97-107.
- Ver Ploeg M, et al. Access to Affordable and Nutritious Food—Measuring and Understanding Nutrient Deserts and Their Consequences: Study to Congress. Washington, DC: U.South. Department of Agronomics, 2009.
- Grimm KA, et al. Admission to Health Nutrient Retailers—Unites States, 2011. CDC Wellness Disparities and Inequalities Written report — United States, 2013. Centers for Disease Control. MMWR Morb Mortal Wkly Rep 2013;62: twenty-26.
- Brulle RJ, Pellow DN. Ecology justice: homo health and ecology inequalities. Annu Rev Public Wellness 2006;27:103-24.
- Basch CE. Healthier Students Are Better Learners: A Missing Link in Schoolhouse Reforms to Close the Achievement Gap. New York: Columbia University, 2010.
- Case A, et al. The lasting impact of childhood health and circumstance. J Wellness Econ 2005;24:365-89.
- Suhrcke Thousand, de Paz Nieves C. The impact of wellness and wellness behaviours on educational outcomes in loftier-income countries: a review of the evidence. Copenhagen, WHO Regional Office for Europe, 2011.
- Barbaresi WJ, et al. Long-term school outcomes for children with attention-deficit/hyperactivity disorder: a population-based perspective. J Dev Behav Pediatr 2007;28:265-73.
- Behrman JR, Rosenzweig MR. 2004. Returns to birthweight. Rev Econ Statistics 2004;86:586-601.
- Black SE. et al. From the Cradle to the Labor Market place? The Issue of Birth Weight on Developed Outcomes. NBER Working Papers 11796, National Agency of Economic Research, 2005.
- Avchen RN, et al. Birth weight and school-age disabilities: a population-based study. Am J Epidemiol 2002;154:895-901.
- Chapman DA, et al. Public health approach to the written report of mental retardation. Am J Ment Retard 2008;113:102-16.
- Conti G, Heckman JJ. Understanding the early origins of the instruction-health gradient. Perspect Psychol Sci 2010;5:585-605.
- Denhem SA. Social-emotional competence as back up for school readiness: what is information technology and how do we appraise It? Early Educ Dev 2006;17:57-89.
- Williams Shanks TR, Robinson C. Assets, economic opportunity and toxic stress: a framework for understanding kid and educational outcomes. Econ Educ Rev 2013;33:154-lxx.
- Currie J. Good for you, wealthy, and wise: socioeconomic status, poor health in childhood, and human being capital letter development. J Econ Lit 2009,47:87–122.
- Leventhal T, Brooks-Gunn J. The neighborhood they live in: the effects of neighborhood residence on kid and boyish outcomes. Psychol Bull 2000;126:309-337.
- Barnett WS, Belfield CR. Early babyhood evolution and social mobility. Future Kid 2006;16:73-98.
- Hackman DA, et al. Socioeconomic condition and the brain: mechanistic insights from human and beast research. Nat Rev Neurosci 2010;eleven:651-9.
- Gottesman II, Hanson DR. Homo development: biological and genetic processes. Annu Rev Psychol 2005;56:263-86.
- Shonkoff JP, Phillips DA, Eds. From Neurons to Neighborhoods: The Science of Early on Child Development. National Inquiry Council and Establish of Medicine. Washington, DC: The National Academies Printing, 2000.
- Felitti VJ, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Babyhood Experiences (ACE) Written report. Am J Prev Med 1998;14:245-58.
- McEwen BS. Brain on stress: how the social surroundings gets under the skin. Proc Natl Acad Sci 2012;109 Suppl 2:17180-5
- Zhang TY, Meaney MJ. Epigenetics and the environmental regulation of the genome and its function. Annu Rev Psychol 2010;61:439-66.
- Egerter Due south, et al. Education and Health. Robert Wood Johnson Foundation, 2011.
- Mistry KB, et al. A new framework for childhood health promotion: the role of policies and programs in edifice capacity and foundations of early childhood health. Am J Public Health 2012;102:1688-96.
- Liu Y, et al. Relationship betwixt adverse babyhood experiences and unemployment among adults from v U.S. states. Soc Psychiatry Psychiatr Epidemiol 2013;48:357-69.
- Williams DR, Mohammed SA. Discrimination and racial disparities in wellness: Evidence and needed inquiry. J Behav Med 2009;32(one), 20–47.
- White K, Borrell LN. Racial/ethnic residential segregation: Framing the context of health risk and health disparities. Health Place 2011;18: 438-48.
- Smedley BD et al., eds. Unequal Treatment: Against Racial and Ethnic Disparities in Health Care. Washington, DC: The National Academies Press, 2003.
Source: https://societyhealth.vcu.edu/work/the-projects/why-education-matters-to-health-exploring-the-causes.html
0 Response to "Despite Reading Numerous Research Studies That Report the Association of Fast Food"
Post a Comment